
A Síndrome de disgenesia gonadal: a Disgenesia gonadal é um distúrbio do desenvolvimento gonadal (testículos ou ovários). Em pacientes que apresentam cariótipo normal, é chamada de disgenesia gonadal pura. Sendo a produção de hormônios sexuais prejudicada, em mulheres a disgenesia gonadal é causa de infantilismo sexual e amenorréia. No passado, pacientes com a síndrome de disgenesia gonadal frequentemente não recebiam terapia de reposição estrogênica até depois dos 13 anos de idade devido ao temor de comprometer a estatura adulta. No entanto, a terapia de estrogênio em baixas doses (de 5 a 10 g de etinilestradiol por via oral) pode ser administrada para permitir a feminilização e melhorar o status psicológico com 12 ou 13 anos de idade sem reduzir a estatura final, conforme demonstrado em vários estudos. O estrogênio em baixas doses aumenta a velocidade de crescimento, enquanto estrogênios em altas doses a suprime. Mesmo que a velocidade de crescimento seja aumentada, no entanto, a estatura adulta não é aumentada com esse tratamento. O tratamento da síndrome de Turner com GH aumenta com sucesso a estatura da idade adulta. Durante a infância estas meninas devem ser regularmente rastreadas para estrabismo, perda auditiva e doença autoimune da tireóide, p. ex., moléstia de Hashimoto bem como dificuldades de aprendizado.


- A síndrome de Turner e suas variações (ou seja, mosaicismo);
- Disgenesia gonadal XX, também pura disgenesia gonadal, 46, XX;
- Síndrome Swyer, disgenesia gonadal também pura, 46, XY;
- Síndrome de Perrault, XX disgenesia gonadal + perda auditiva neurossensorial;
- Disgenesia gonadal mista;
- A exposição ao meio ambiente dos desreguladores endócrinos.
É de extrema importância efetuar o diagnóstico e estabelecer a terapêutica o mais precoce possível.

CHILD, INFANTILE, JUVENILE WITH COMMITTAL DEVELOPMENT COMMITTAL: SYNDROME GONADAL DYSGENESIS EVIDENT AND COMMITMENT IN HEIGHT GROWTH (HEIGHT).
GROWING CHILD, YOUTH AND PUBERTAL, COMMITTED SECONDARILY: A HORMONE DEFICIENCY ACCOMPANYING ALSO PREVENTS THE DEVELOPMENT OF SECONDARY SEXUAL CHARACTERISTICS IN BOTH SEXES, RESULTING IN AN APPEARANCE OF FEMALE CHILD SEXUALLY INFERTILITY. PHYSIOLOGY-ENDOCRINOLOGY, NEUROENDOCRINOLOGY-GENETICS-ENDOCRINE-PEDIATRICS (SUBDIVISION OF ENDOCRINOLOGY):
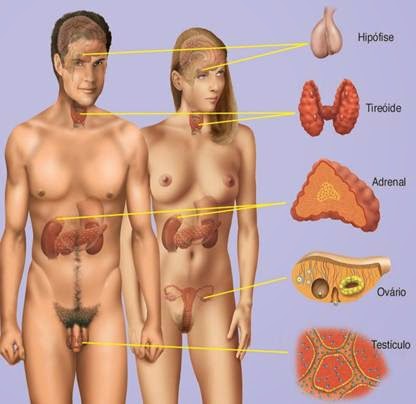 IN BOTH SEXES, THE BEGINNING AND PROGRESSION OF PUBERTY REQUIRE GONADS FUNCTIONAL, WORKING IN HARMONY WITH GLANDS HYPOTHALAMIC AND PRODUCING PITUITARY HORMONES ENOUGH. FOR THIS REASON, GONADAL DYSGENESIS FAILURE IN HORMONE THAT SHIPPED ALSO PREVENTS THE DEVELOPMENT OF SECONDARY SEXUAL CHARACTERISTICS IN BOTH SEXES, RESULTING IN AN APPEARANCE AND FEMALE CHILD SEXUALLY INFERTILITY, INCLUDING GROWTH DEFICIENCY. DR. JOÃO SANTOS CAIO JR. ET DRA. HENRIQUETA VERLANGIERI CAIO.
IN BOTH SEXES, THE BEGINNING AND PROGRESSION OF PUBERTY REQUIRE GONADS FUNCTIONAL, WORKING IN HARMONY WITH GLANDS HYPOTHALAMIC AND PRODUCING PITUITARY HORMONES ENOUGH. FOR THIS REASON, GONADAL DYSGENESIS FAILURE IN HORMONE THAT SHIPPED ALSO PREVENTS THE DEVELOPMENT OF SECONDARY SEXUAL CHARACTERISTICS IN BOTH SEXES, RESULTING IN AN APPEARANCE AND FEMALE CHILD SEXUALLY INFERTILITY, INCLUDING GROWTH DEFICIENCY. DR. JOÃO SANTOS CAIO JR. ET DRA. HENRIQUETA VERLANGIERI CAIO.

Gonadal dysgenesis syndrome: in the past, patients with the syndrome of gonadal dysgenesis often not receiving estrogen replacement therapy until after the age of 13 due to fear of compromising adult height. However, estrogen therapy at low doses (from 5 to 10 g ethinyl estradiol administered orally) can be administered to allow feminization and improve the psychological status in 12 or 13 years of age without reducing the final height, as shown in several studies. The low dose estrogen increases the rate of growth, while high-dose estrogen suppresses. Even though the growth rate is increased, however, the adult height is not increased with this treatment. The treatment of Turner syndrome with GH increases the stature of successful adulthood. During childhood these girls should be regularly screened for strabismus, hearing loss and autoimmune thyroid disease, e. g., Hashimoto's disease and learning disabilities. There are several recommendations for preparing these transition for girls in adults care required for monitoring aspects that affect their later life, including monitoring the development of aortic dilatation at intervals of 5 to 10 years since this defect can progress to the appearance of aortic aneurysms. Changes of this gonadal dysgenesis syndrome are more you frequent in such causes:
Site Van Der Häägen Brazil
www.vanderhaagenbrazil.com.br
http://drcaiojr.site.med.br
http://dracaio.site.med.br
João Santos Caio Jr
http://google.com/+JoaoSantosCaioJr
Vídeo
http://youtu.be/woonaiFJQwY
Google Maps:
http://maps.google.com.br/maps/place?cid=5099901339000351730&q=Van+Der+Haagen+Brasil&hl=pt&sll=-23.578256,46.645653&sspn=0.005074,0.009645&ie=UTF8&ll=-23.575591,-46.650481&spn=0,0&t = h&z=17

CHILD, INFANTILE, JUVENILE WITH COMMITTAL DEVELOPMENT COMMITTAL: SYNDROME GONADAL DYSGENESIS EVIDENT AND COMMITMENT IN HEIGHT GROWTH (HEIGHT).
GROWING CHILD, YOUTH AND PUBERTAL, COMMITTED SECONDARILY: A HORMONE DEFICIENCY ACCOMPANYING ALSO PREVENTS THE DEVELOPMENT OF SECONDARY SEXUAL CHARACTERISTICS IN BOTH SEXES, RESULTING IN AN APPEARANCE OF FEMALE CHILD SEXUALLY INFERTILITY. PHYSIOLOGY-ENDOCRINOLOGY, NEUROENDOCRINOLOGY-GENETICS-ENDOCRINE-PEDIATRICS (SUBDIVISION OF ENDOCRINOLOGY):

Gonadal dysgenesis syndrome: in the past, patients with the syndrome of gonadal dysgenesis often not receiving estrogen replacement therapy until after the age of 13 due to fear of compromising adult height. However, estrogen therapy at low doses (from 5 to 10 g ethinyl estradiol administered orally) can be administered to allow feminization and improve the psychological status in 12 or 13 years of age without reducing the final height, as shown in several studies. The low dose estrogen increases the rate of growth, while high-dose estrogen suppresses. Even though the growth rate is increased, however, the adult height is not increased with this treatment. The treatment of Turner syndrome with GH increases the stature of successful adulthood. During childhood these girls should be regularly screened for strabismus, hearing loss and autoimmune thyroid disease, e. g., Hashimoto's disease and learning disabilities. There are several recommendations for preparing these transition for girls in adults care required for monitoring aspects that affect their later life, including monitoring the development of aortic dilatation at intervals of 5 to 10 years since this defect can progress to the appearance of aortic aneurysms. Changes of this gonadal dysgenesis syndrome are more you frequent in such causes:
- Turner syndrome and its variants (e.g., mosaicism);
- Gonadal dysgenesis XX also pure gonadal dysgenesis, 46, XX;
- Swyer syndrome, also pure gonadal dysgenesis 46, XY;
- Perrault syndrome, gonadal dysgenesis XX + sensorineural hearing loss;
- Mixed gonadal dysgenesis;
- Exposure to environmental endocrine disrupting chemicals.
It is very important to make early diagnosis and precoces therapeutic potential.
Como saber mais:
1. Quando for citada a utilização de roedores, provavelmente os humanos irão se comportar muito proximamente sob o aspecto orgânico e metabólico, e as conclusões científicas advirão desses passos vitais. Camundongos mutantes que têm tanto falta de IGF-1 (IGF-1, fator de crescimento semelhante à insulina-1) quanto de receptores de GH têm apenas 17% do tamanho normal...
http://hormoniocrescimentoadultos.blogspot.com
2. Essas observações indicam que tanto o (IGF-1, fator de crescimento semelhante à insulina-1) quanto o (IGF-2, fator de crescimento semelhante à insulina-2) são fatores embriônico e de crescimento fetais importantes, mas que o GH sozinho também tem um papel modesto independente do IGF e este fato é mais evidente nos fetos...
http://longevidadefutura.blogspot.com
3. Mesmo que o tamanho fetal tenha sido proporcionalmente reduzido em ambas as situações e mesmo que a morfogênese estivesse inteiramente normal, uma taxa de mortalidade maior no neonato foi observada após a ruptura do gene do IGF-1. O atraso no crescimento começou no 11º dia para nockaute de IGF-2 e no 13.5º dia para knockoute de IGF-1...
http://imcobesidade.blogspot.com
AUTORIZADO O USO DOS DIREITOS AUTORAIS COM CITAÇÃO
DOS AUTORES PROSPECTIVOS ET REFERÊNCIA BIBLIOGRÁFICA.
Referências Bibliográficas:
Caio Jr, João Santos, Dr.; Endocrinologista, Neuroendocrinologista, Caio,H. V., Dra. Endocrinologista, Medicina Interna – Van Der Häägen Brazil, São Paulo, Brasil; Mauras N, Rogol AD, Veldhuis JD. Increased hGH production rate after low-dose estrogen therapy in prepubertal girls with Turner’s syndrome. Pediatr Res. 1990;28:626–630; Tanner JM. Growth at adolescence. 2nd ed. Oxford, England: Blackwell Scientific; 1962; National Center for Health Statistics. Rockville, MD: Health Resources Administration; 1976. NCHS growth charts; Greulich WW, Pyle SI. Radiographic atlas of skeletal development of the hand and wrist. 2nd ed. Stanford, CA: Stanford University Press; 1959; Kuczmarski RJ, Ogden CL, Grummer-Strawn LM, et al. Advance data from vital and health statistics. Hyattsville, MD: National Center for Health Statistics; 2000. CDC growth charts: United States. No. 246; Tanner JM, Whitehouse RH, Hughes PC, Vince FP. Effect of human growth hormone treatment for 1 to 7 years on growth of 100 children, with growth hormone deficiency, low birthweight, inherited smallness, Turner’s syndrome, and other complaints. Arch Dis Child. 1971;46:745–782; Siddiqui O, Hung HMJ, O’Neill R. MMRM vs. LOCF: a comprehensive comparison based on simulation study and 25 NDA datasets. J Biopharm Stat. 2009;19:227–246; Sacks H, Chalmers TC, Smith H., Jr Randomized versus historical controls for clinical trials. Am J Med. 1982;72:233–240; Hopwood NJ, Hintz RL, Gertner JM, et al. Growth response of children with non-growth-hormone deficiency and marked short stature during three years of growth hormone therapy. J Pediatr. 1993;123:215–222; Nilsson O, Marino R, De Luca F, Phillip M, Baron J. Endocrine regulation of the growth plate. Horm Res. 2005;64:157–165; Klein KO, Baron J, Colli MJ, McDonnell DP, Cutler GB., Jr Estrogen levels in childhood determined by an ultrasensitive recombinant cell bioassay. J Clin Invest. 1994;94:2475–2480; Courant F, Aksglaede L, Antignac J-P, et al. Assessment of circulating sex steroid levels in prepubertal and pubertal boys and girls by a novel ultrasensitive gas chromatography-tandem mass spectrometry method. J Clin Endocrinol Metab. 2010;95:82–92; Rosenfield RL, Devine N, Hunold JJ, Mauras N, Moshang T, Jr, Root AW. Salutary effects of combining early very low-dose systemic estradiol with growth hormone therapy in girls with Turner syndrome. J Clin Endocrinol Metab. 2005;90:6424–6430; Soriano-Guillen L, Coste J, Ecosse E, et al. Adult height and pubertal growth in Turner syndrome after treatment with recombinant growth hormone. J Clin Endocrinol Metab. 2005;90:5197-–5204.
Dr. João Santos Caio Jr.
Endocrinologia – Neuroendocrinologista
CRM 20611
Dra. Henriqueta V. Caio
Endocrinologista – Medicina Interna
CRM 28930
1. Quando for citada a utilização de roedores, provavelmente os humanos irão se comportar muito proximamente sob o aspecto orgânico e metabólico, e as conclusões científicas advirão desses passos vitais. Camundongos mutantes que têm tanto falta de IGF-1 (IGF-1, fator de crescimento semelhante à insulina-1) quanto de receptores de GH têm apenas 17% do tamanho normal...
http://hormoniocrescimentoadultos.blogspot.com
2. Essas observações indicam que tanto o (IGF-1, fator de crescimento semelhante à insulina-1) quanto o (IGF-2, fator de crescimento semelhante à insulina-2) são fatores embriônico e de crescimento fetais importantes, mas que o GH sozinho também tem um papel modesto independente do IGF e este fato é mais evidente nos fetos...
http://longevidadefutura.blogspot.com
3. Mesmo que o tamanho fetal tenha sido proporcionalmente reduzido em ambas as situações e mesmo que a morfogênese estivesse inteiramente normal, uma taxa de mortalidade maior no neonato foi observada após a ruptura do gene do IGF-1. O atraso no crescimento começou no 11º dia para nockaute de IGF-2 e no 13.5º dia para knockoute de IGF-1...
http://imcobesidade.blogspot.com
AUTORIZADO O USO DOS DIREITOS AUTORAIS COM CITAÇÃO
DOS AUTORES PROSPECTIVOS ET REFERÊNCIA BIBLIOGRÁFICA.
Referências Bibliográficas:
Caio Jr, João Santos, Dr.; Endocrinologista, Neuroendocrinologista, Caio,H. V., Dra. Endocrinologista, Medicina Interna – Van Der Häägen Brazil, São Paulo, Brasil; Mauras N, Rogol AD, Veldhuis JD. Increased hGH production rate after low-dose estrogen therapy in prepubertal girls with Turner’s syndrome. Pediatr Res. 1990;28:626–630; Tanner JM. Growth at adolescence. 2nd ed. Oxford, England: Blackwell Scientific; 1962; National Center for Health Statistics. Rockville, MD: Health Resources Administration; 1976. NCHS growth charts; Greulich WW, Pyle SI. Radiographic atlas of skeletal development of the hand and wrist. 2nd ed. Stanford, CA: Stanford University Press; 1959; Kuczmarski RJ, Ogden CL, Grummer-Strawn LM, et al. Advance data from vital and health statistics. Hyattsville, MD: National Center for Health Statistics; 2000. CDC growth charts: United States. No. 246; Tanner JM, Whitehouse RH, Hughes PC, Vince FP. Effect of human growth hormone treatment for 1 to 7 years on growth of 100 children, with growth hormone deficiency, low birthweight, inherited smallness, Turner’s syndrome, and other complaints. Arch Dis Child. 1971;46:745–782; Siddiqui O, Hung HMJ, O’Neill R. MMRM vs. LOCF: a comprehensive comparison based on simulation study and 25 NDA datasets. J Biopharm Stat. 2009;19:227–246; Sacks H, Chalmers TC, Smith H., Jr Randomized versus historical controls for clinical trials. Am J Med. 1982;72:233–240; Hopwood NJ, Hintz RL, Gertner JM, et al. Growth response of children with non-growth-hormone deficiency and marked short stature during three years of growth hormone therapy. J Pediatr. 1993;123:215–222; Nilsson O, Marino R, De Luca F, Phillip M, Baron J. Endocrine regulation of the growth plate. Horm Res. 2005;64:157–165; Klein KO, Baron J, Colli MJ, McDonnell DP, Cutler GB., Jr Estrogen levels in childhood determined by an ultrasensitive recombinant cell bioassay. J Clin Invest. 1994;94:2475–2480; Courant F, Aksglaede L, Antignac J-P, et al. Assessment of circulating sex steroid levels in prepubertal and pubertal boys and girls by a novel ultrasensitive gas chromatography-tandem mass spectrometry method. J Clin Endocrinol Metab. 2010;95:82–92; Rosenfield RL, Devine N, Hunold JJ, Mauras N, Moshang T, Jr, Root AW. Salutary effects of combining early very low-dose systemic estradiol with growth hormone therapy in girls with Turner syndrome. J Clin Endocrinol Metab. 2005;90:6424–6430; Soriano-Guillen L, Coste J, Ecosse E, et al. Adult height and pubertal growth in Turner syndrome after treatment with recombinant growth hormone. J Clin Endocrinol Metab. 2005;90:5197-–5204.
Contato:
Fones: 55 (11) 2371-3337 - 5572-4848 ou 9.8197-4706
Rua Estela, 515 - bloco D - 12º andar - conj 121 e 122 - Paraiso - São Paulo - SP - CEP 04011-002
email: vanderhaagenbrasil@gmail.com
Rua Estela, 515 - bloco D - 12º andar - conj 121 e 122 - Paraiso - São Paulo - SP - CEP 04011-002
email: vanderhaagenbrasil@gmail.com
www.vanderhaagenbrazil.com.br
http://drcaiojr.site.med.br
http://dracaio.site.med.br
João Santos Caio Jr
http://google.com/+JoaoSantosCaioJr
Vídeo
http://youtu.be/woonaiFJQwY
Google Maps:
http://maps.google.com.br/maps/place?cid=5099901339000351730&q=Van+Der+Haagen+Brasil&hl=pt&sll=-23.578256,46.645653&sspn=0.005074,0.009645&ie=UTF8&ll=-23.575591,-46.650481&spn=0,0&t = h&z=17